
08 Nov Thin Endometrium
Endometrial PRP / Endometrial PL Rejuvenation / Endometrial Stem Cells Infusion / GCSF
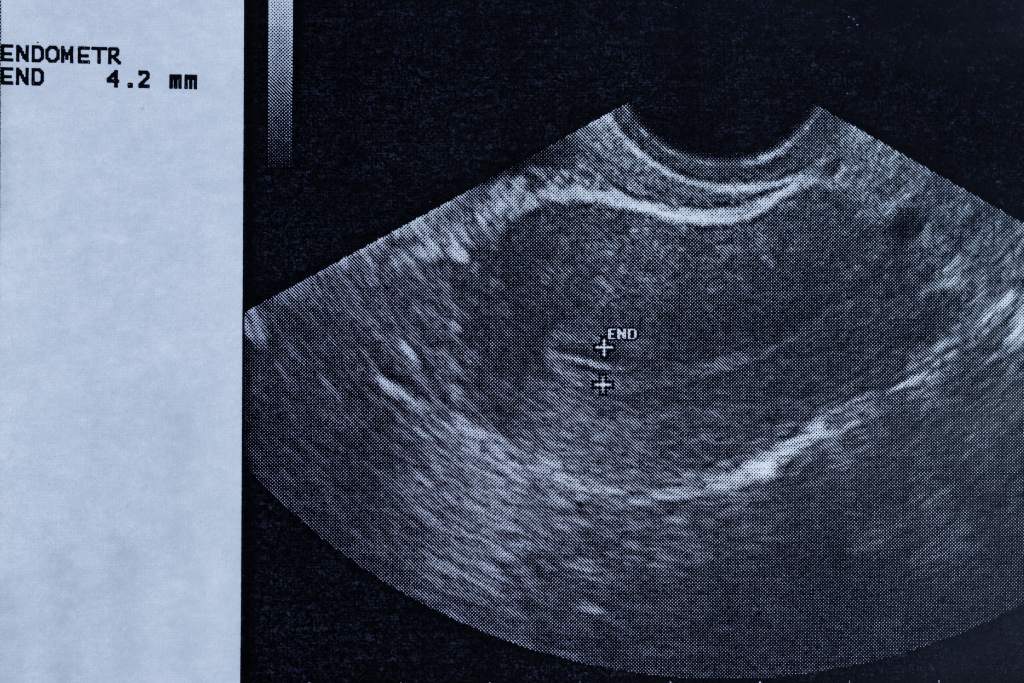
Endometrium thickness or actually non – thickness issue, is one of the most difficult ones in reproductive medicine. Endometrium, due to the lack of oestrogen, is always thin in menopausal women. In that case, hormonal oestrogen pretreatment, helps to increase the thickness, so that an early pregnancy will be supported.
Many times though, endometrium does not get thick in women with normal menstrual cycles too. In natural cycles or even medicated cycles.
When endometrium does not get thick, this is usually a difficult issue to deal with :
Why endometrium does not get thick ?
• Reaction to long time use of contraceptive pill or GNRH down reg injections that many times are used in frozen embryo transfer protocols, to prevent ovulation. In cases like these, change of protocol to letrazole induced frozen cycles, natural frozen cycles or modified naturals, might help diagnose if the problem will persist
or not. Daily oestrogen use in doses more than 8 mg, has not been proved to add any benefit. Transdermal or even vaginal oestrogen might help.
• Intrauterine adhesions (scar tissue), due to past surgeries like terminations, D&Cs, myomectomies etc or infections (endometritis), PID etc. In cases like that, hysteroscopic surgical correction is the 1st line treatment. Repeated surgeries might be needed and aditional oestrogen treatments. Even if the scar tissue is finally
corrected, there are usually no guarantees that the restored endometrium will be healthy on a cell level and thickness might continue to be an issue, even after
multiple surgeries.
• Chronic endometritis, due to past infections, might cause persistent thin endometrium, with or without adhesions. A diagnostic hysteroscopy, when that is performed by an experienced reproductive medicine specialist, can make a diagnosis. Endometrial biopsies and analysis in molecular level, can confirm the diagnosis. Triple antibiotic scheme for at least 10 days, might help grossly in the subsequent thickness of the endometrium. There is no conclusive evidence that
intrauterine infusions of antibiotics, help more than oral treatment.
• No obvious reason (? Immunological) What happens though, when endometrium remains thin, with no obvious reason or surgical treatments and antibiotic treatments, have not worked? This is where novel add on treatments, like endometrial PRP, stem cells infusion or GCF or combination of the above might help.
Endometrial PRP
Platelet rich plasma (double centrifugated) is injected inside the endometrium, with the help of a catheter, as an outpatient simple procedure that is quite similar with the embryo transfer. That, especially when is associated with an endometrial scratching, can activate regenarative endometrial stem cells and create new vessels and cytokines that help grossly with the endometrial thickness. If cervical canal is stenosed, same procedure can also be done under sedation or even be combined with a hysteroscopy. We usually prefer to use this technique when endometrium remains thin after surgical correction of mild scar tissue or antibiotic treatment.
PL Endometrial Rejuvenation
With this novel technique the blood drawn from the forearm is centrifugated in a much stronger machine. That results, in complete separation of each component, breaking down of the platelets in the plasma due to Platelet Lysate activation and collection and concentration of an enriched autologus mixture of growth factors and cytokines. Concentration of these is supposed to be 10- 15 times more than usually. As a result endometrial rejuvenation might be quicker and last longer. Procesur can be done either as an out patient or under sedation or even combined with a hysteroscopy. We now prefer to use this technique, in cases of mild to medium Asherman’ s or previously treated chronic endometritis cases.
Stem Cells Infusion \ PL endometrial rejuvenation
Fat tissue is collected with a minor incision on the tummy. This is centrifugated and developped in a culture for about one month, with the aim to create adipose derived stem cells. These are combined with a PL mixture and are injected below the endometrium, preferrably under hysteroscopic guidance. This technique is a novel and pioneered one, that is usually applied in very difficult persistent cases of Severe Asherman’ s history etc.
GCSF
GCSF is a glycoprotein and haematopoietic growth factor that regulates the formation of neutrophils, which are white blood cells, that are increased in inflammation and infections.
It has been found out that it does help the formation of micro vessels in the endometrium, increasing the blood flow. Also might affect implantation by alternating local inflammation factors like macrophages. On many studies, has been shown that it helps in increasing the thickness of the endometrium. Even when thickness is not a main issue, on many unexplained failures of implantation, with possible local immunological aetiology, GCSF increase the pregnancy rate. We use GCSF when we have unexplained reduced thickness of the endometrium or borderline thickness or in cases of unexplained failures of implantation or immunological local contributing factors. Can sometimes also be used on a combination with PL endometrial rejuvenation infusions in difficult multifactor aetiology’ s cases. We call this potent endometrial infusion, Forte Mixture.
No Comments